The CSANZ Board is reviewing the strategic priorities for the society. A short survey was prepared in March 2023 to inform the Board about what areas you consider important that should be prioritised and resourced. The results were published in the April 2023 edition of On the Pulse.
ON THE PULSE APRIL 2023
Editorial by Prof Will Parsonage. (link to pdf)
In its 70 year history the Cardiac Society of Australia and New Zealand (CSANZ) has grown from a small group of 47 interested physicians and surgeons to a community of nearly 2,400 members spanning all the professional groups essential to the delivery of modern, multidisciplinary healthcare for people and communities with cardiac disease.
CSANZ will always hold true to its constitutional aim of ‘promoting the highest standards of education, training, research and practice in cardiovascular medicine and surgery’ but recognises the importance of incorporating this in line with the thoughts, beliefs and priorities of its broader membership.
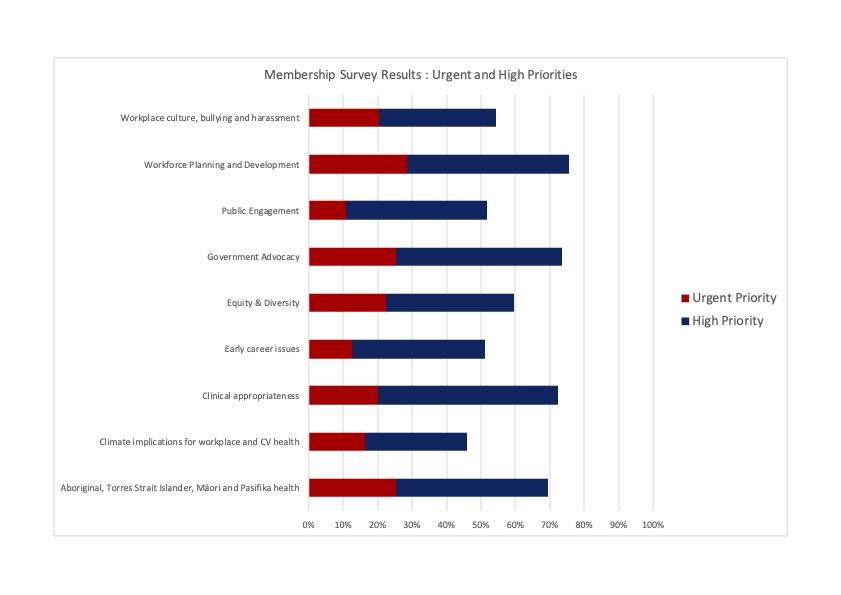
The board are frequently approached by members regarding a broad range of issues that apply to this context. We recently conducted a survey to gauge the priority that members attach to several of these. The aim of the survey was not to rigidly define strategic priorities for the society but rather to ‘take the pulse’ of the wider membership on some of the issues more frequently raised by individuals.
Responses were received from over 300 members about 60% of whom were medical staff and around 15% nursing staff. New Zealand and all states and territories of Australia were represented. Although one respondent felt that the survey had ‘missed the mark’ in the selection of priorities that were presented all were considered to be of urgent or high priority by at least 40% of those who participated. Four areas were considered to be of urgent or high priority by more than two-thirds, namely; health of First Nation peoples, clinical appropriateness, government advocacy and workplace planning and development.
Members were also generous with personal views given the opportunity to provide individual comments. These provided a rich source of additional insights beyond the quantitative aspects of the survey. Above all, these emphasise the challenge that a society with broad membership faces in attempting to meet the needs of all.
‘What about planetary health that was brought up… at our AGM?’ (Anon. A)
‘Members who want to be effective… (in these areas) …should be encouraged to join a political party rather than the cardiac society’ (Anon. B)
In considering the outcomes of the survey the leadership of the Society are conscious that we have a limited capacity to ‘change the world’ and that there is a risk in spreading our resources too thinly, achieving nothing and even losing sight of our core purpose. In some areas it may be enough for the Society to state a position and work in support of others to achieve a common goal. In others the society can take a more active role in facilitating change.
The Society are grateful to all those who took the time to complete the survey but we are conscious that, like all surveys of this kind, the outcomes still only reflect the views of a self-selected group of our members. With that in mind we see the survey not as a final word but the beginning of a conversation out of which the Society can move forward in the future better informed about what matters to our members.
For those interested a more detailed presentation of the survey results will be made at the annual general meeting of the society at this year’s annual scientific meeting in Adelaide Board members and state based representatives are always happy to be approached by members to discuss society business. If you are not sure who to contact in representing your region or professional group details of members of the Board (who include representatives of New Zealand and every Australian State) and Councils can be found on the Society website at csanz.edu.au