The CSANZ Indigenous Health Prize will be awarded to the best individual presentation in the Indigenous Health Prize session at the 2023 Annual Scientific Meeting.
Abstracts are invited for studies involving Aboriginal, Torres Strait Islander, Māori or Pacific Islander populations. Applications will need to demonstrate engagement with Indigenous leadership, community members or Indigenous stakeholders during the research process, and the contribution of the research to reducing inequity and delivering tangible benefits for communities.
Click here for all the prize details, submission requirements and how to apply.
Applications close on Monday, 8 May 2023
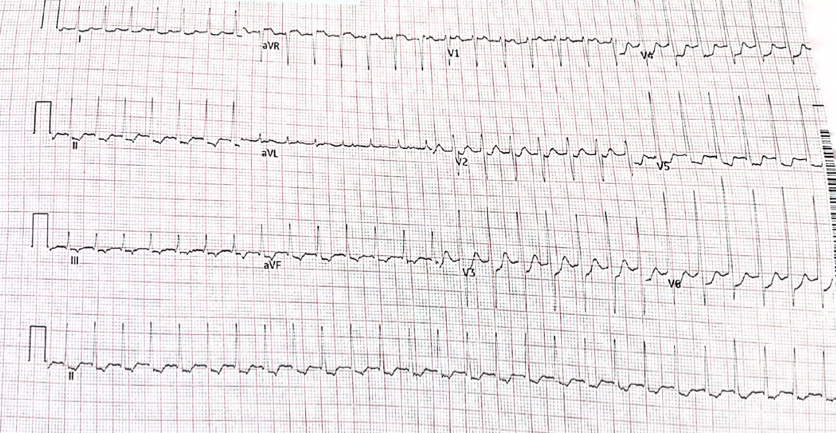
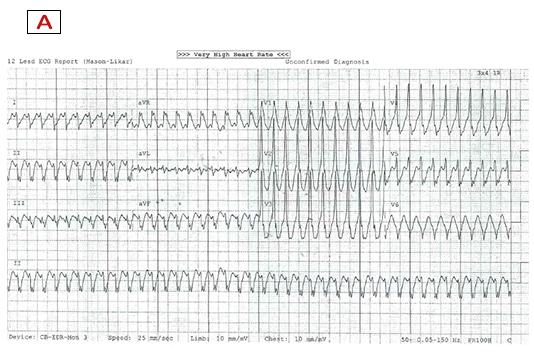
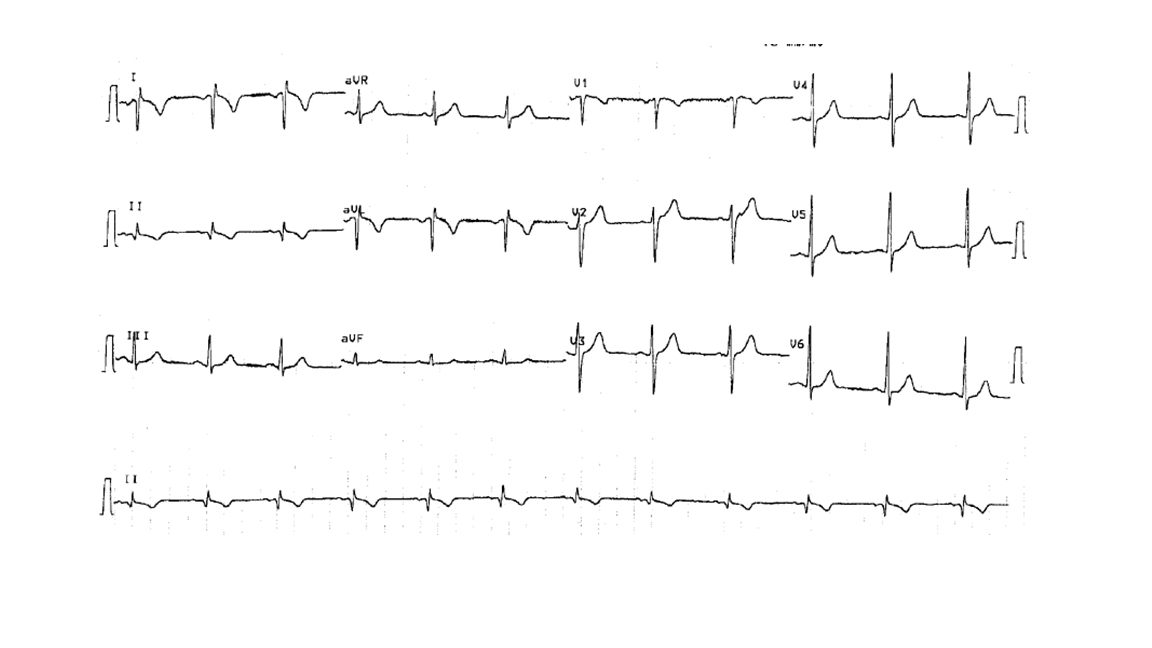
A 72 year old woman presents with palpitations and pre-syncope. Initial ECGs is shown below (Figure 1):
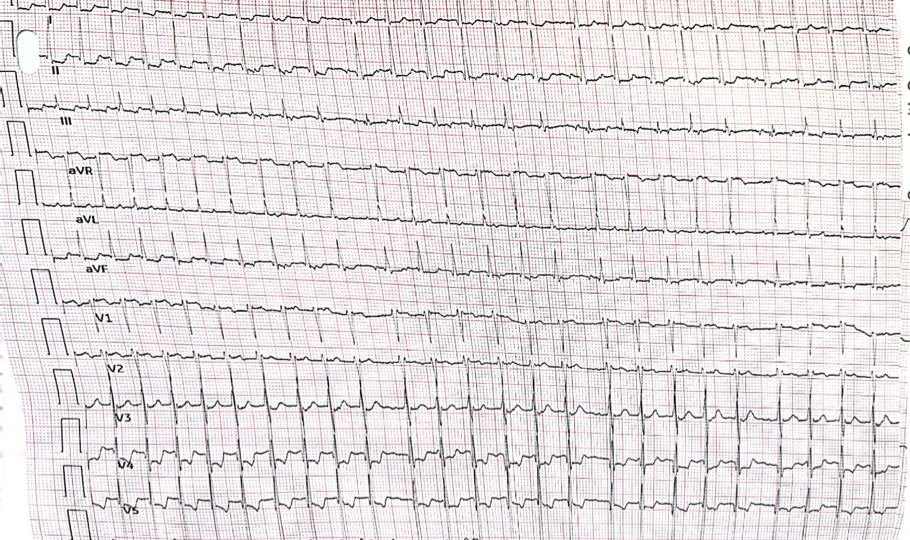
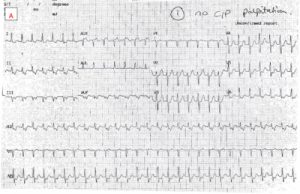
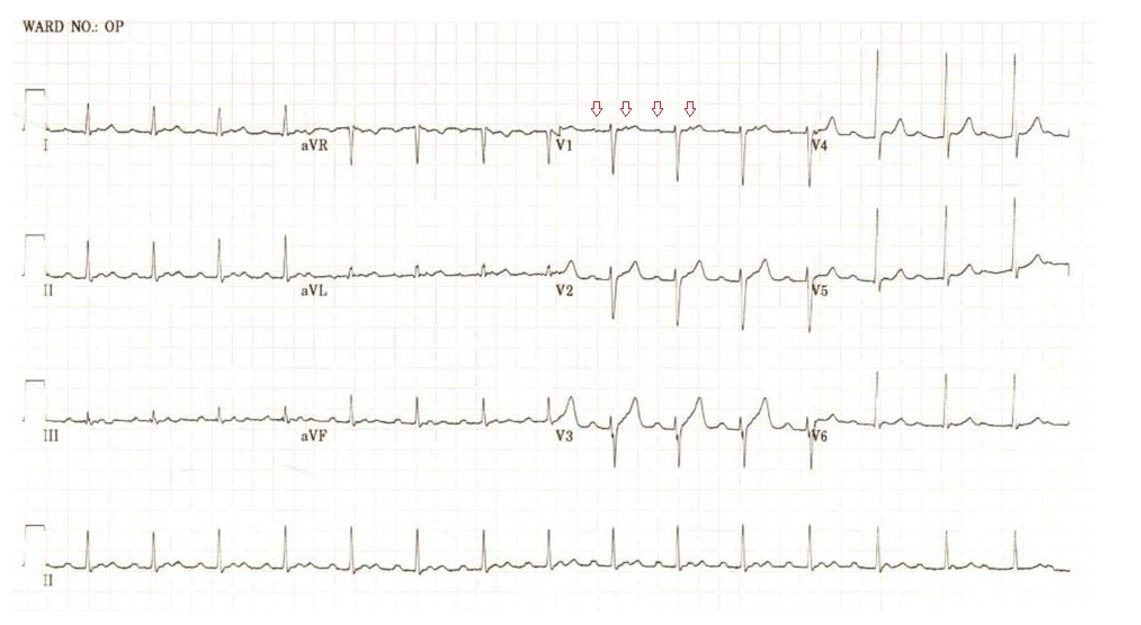
A Valsalva manoeuvre is attempted and subsequent ECG is shown below (Figure 2):
What is the most likely diagnosis? Want to ask a question or discuss visit the ECG Forum…
Answer:
Atrial tachycardia with Wenckebach AV nodal conduction.
Explanation:
The initial ECG demonstrates a ‘short RP’ SVT with the p-wave best seen in lead aVL on the initial ECG. The differentials are typical atrioventricular nodal reentrant tachycardia (usually the retrograde p wave is buried at the end of the QRS which is not the case here), atrioventricular reentrant tachycardia or atrial tachycardia (AT) with first degree AV block.
The second ECG following a ‘vagal’ manoeuvre does not terminate the tachycardia but increases the block at the level of the AV node. This exposes the p-waves and there are more ‘A’s than ‘V’s with grouped beating seen (best appreciated in lead III). This Wenckebach pattern excludes AVRT (in fact by definition the A:V relationship must be 1:1) and makes AVNRT very unlikely. The p-wave morphology is nearly isoelectric in V1 and very ‘skinny’ suggesting a mid-line origin. In pact at EP study the focal atrial tachycardia was mapped to the perinodal region and successfully ablated there.

In this edition:
– Cryoablation vs drug therapy for paroxysmal AF
– Myopericarditis after COVID-19 mRNA vaccination
– Rate of progression of aortic stenosis
– Metformin can be safely used in patients exposed to contrast media
– Use of bempedoic acid in statin-intolerant patients
– Effects of dapagliflozin in heart failure patients with or without gout
– SGLT2 inhibitors and cancer outcomes
– Overweight or obesity increases the risk of cardiovascular disease
– Efficacy and safety of the oral PCSK9 inhibitor MK-0616
– Inflammation and cholesterol as predictors of cardiovascular events in patients taking statins
Download Cardiology Research Review, Issue 152, with commentary by A/Prof John Amerena (pdf)

In this edition:
– All-cause mortality for torsemide vs. furosemide after HF hospitalisation
– Is exercise capacity limited by elevated PCWP in HFPEF?
– Association of anthracycline exposure with HF
– Sociodemographic differences in HFREF medical therapy
– Effects of His bundle pacing on HF symptoms and exercise capacity
– Cost effectiveness of immediate dapagliflozin in patients with HF history
– Association of PCSK9 loss-offunction variants with HF risk
– Transcriptomic and proteomic profiles identify HF patients with potential for myocardial recovery
– Prognostic implications of PVP-assessed post-discharge haemodynamic congestion after acute HF
– Sex differences in response to dapagliflozin for HF across the EF spectrum

The MBS Heart Health Check is currently due to expire on 30 June 2023, and there are concerns that the Federal Government will not extend this item.
Whilst our partners, the Heart Foundation of Australia and Hearts4heart advocacy efforts appear to have a preliminary result in reversing the government’s decision to cease the Medicare items dedicated to the Heart Health Check.
Until there is something in writing, (such as a pre-budget announcement), there is no guarantee. So, we ask for your support in promoting the Heart Foundation of Australia’s campaign.
Hearts4heart will continue speaking with MPs and Senators, and they anticipate a formal announcement within the next couple of weeks.
In the meantime, we ask if you could get behind this campaign by sharing on social media and signing the petition here.
Dr Jason Harmer
This case is a rare example of cardiac hydatidosis found in a patient in rural NSW, Australia. He was a middle-aged man who initially presented with a ruptured right ventricular hydatid cyst causing an anaphylactoid-like reaction, pulmonary emboli and widespread dissemination of hydatid echinococcus throughout the lung. He survived the cyst rupture and underwent cardiac surgery, but had incomplete resection and experienced progressive cardiopulmonary hydatidosis despite ongoing antihelminthic therapy. He had an array of cardiopulmonary sequelae over his lifespan, including worsening pulmonary hypertension and right heart failure, as well as bone marrow suppression and neutropenic sepsis. This case highlights rare clinical manifestations of cardiac hydatidosis and potential complications of its treatment.
Hydatidosis is caused by ingestion of larvae from the Echinococcus granulosus tapeworm from contaminated food or water supply or by direct contact with infected animals. Hydatid cysts commonly affect the liver or lung; however, cardiac involvement can occur in rare cases (i.e. <2% of all cases of hydatidosis).
Figure 1
Transthoracic echocardiogram: apical 4 chamber view. Intracardiac hydatid cyst.
Apical attachment of a large hydatid cyst to the wall of the RV. The RV chamber is dilated and hypokinetic and the septum is dyskinetic. The distal portion of the hydatid cyst is mobile. The RA is severely dilated and the interatrial septum is displaced due to pressure overload. The tricuspid annulus appears dilated.
Figure 2
Transthoracic echocardiogram: parasternal short axis view. Intracardiac hydatid cyst.
There is a large mass (hydatid cyst) in the RV that appears to be fixed to parts of the interventricular septum. Motion of the interventricular septum is abnormal, in part due to attachment of the mass and from raised pressures in the right heart. Interventricular septal flattening is a sign of raised right heart pressures. This patient has known moderate to severe pulmonary hypertension as a consequence of dissemination of hydatid disease to the lung and pulmonary thromboembolism.
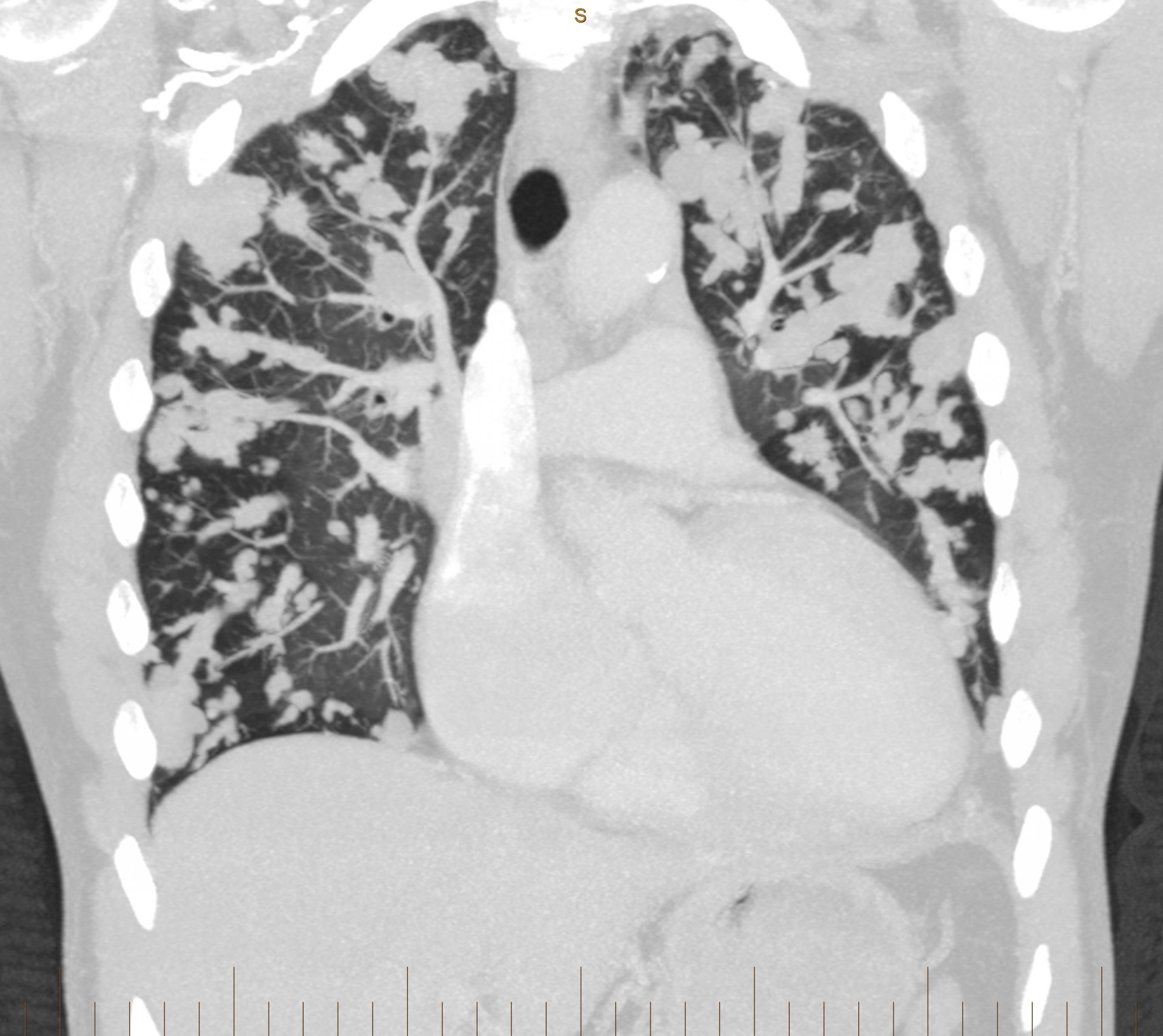
Figure 3
CT pulmonary angiogram: coronal view. Multiple hydatid masses within the pulmonary vasculature.
Multiple lobulated areas within the pulmonary vasculature from extensive dissemination of hydatid disease originating from the RV.
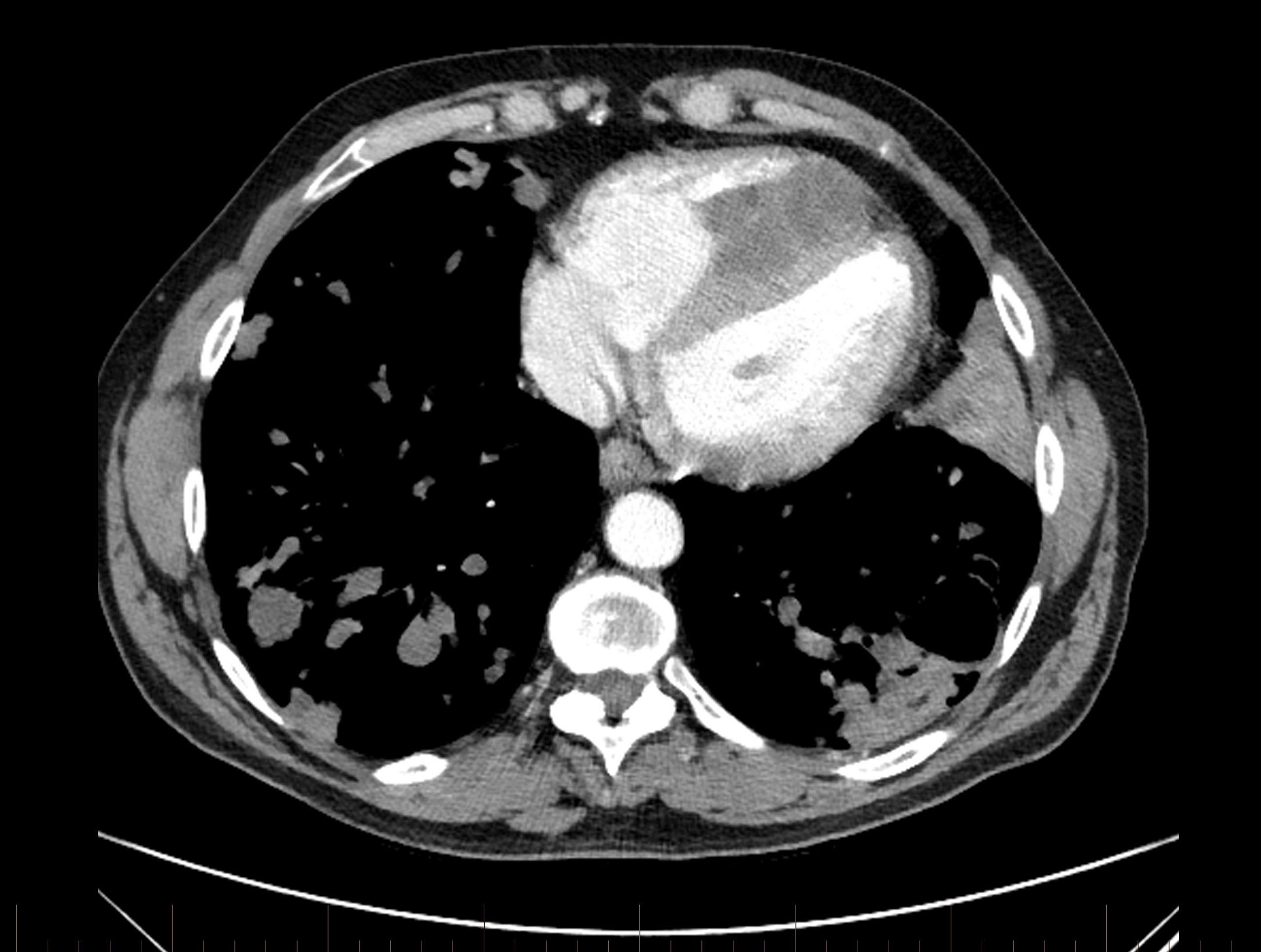
Figure 4
CT pulmonary angiogram: axial view.
There is a dense mass within the RV chamber due to a hydatid cyst. There is reduced RV blood filling in diastole due to the space occupying mass. The interventricular septal wall is clearly demarcated and the mass appears to encroach on the septal wall at two points. The RV is enlarged and occupies the apex of the heart. The sternum has been divided in two parts from a previous stenotomy (with incomplete surgical resection of the mass, leading to regrowth). There is a cavitating lesion in the posterior aspect of the left lung.
Abbrev. CT = computed tomography; RV = right ventricle; LV = left ventricle; RA = right atrium.


