Enjoy the video commentary below presented by A/Prof John Amerena with the highlights of ACC.23.
Enjoy the video commentary below presented by A/Prof John Amerena with the highlights of ACC.23.
The TGA has made a Serious Scarcity Substitution Instrument (SSSI) for warfarin. This instrument is in force until 07 August 2023 and allows a pharmacist to offer the patient or their carer a lower strength of COUMADIN warfarin tablet if the 5mg tablet is unavailable, without prior approval from the prescriber.
The TGA SSSI website provides information to pharmacists, prescribers and patients. The web alert includes a link to a printable PDF patient information sheet that pharmacists may find useful when counselling patients who are dispensed a substitutable medicine. Viatris, the sponsor of COUMADIN tablets will also be disseminating this information sheet.
The substitution has PBS subsidy arrangements, and the PBS website has been updated with this information.
If you have any questions, please contact the Medicine Shortages Section on 02 6289 4646 or email [email protected].

In this issue
– Cardio-oncology recommendations for paediatric oncology
– Myopericarditis after COVID-19 mRNA vaccination
– Circulating spike protein detected in mRNA vaccine-induced myocarditis
– Stepwise approach to prescribing novel lipid-lowering therapy
– Five things physicians and patients should question
– Aortic stenosis progression
– Improved access to PBS medicines for pulmonary arterial hypertension
– Major global coronary artery calcium guidelines
– Renal denervation in the management of hypertension
– Cardiovascular complications of Down syndrome
– Metformin can be safely used in patients exposed to contrast media
– Autopsy rates in all-cause mortality and young sudden death
– COVID-19 resources
– Conferences, workshops and CPD

We are delighted to announce that Prof Julie Sanders, Clinical Professor of Cardiovascular Nursing at Queen Mary University of London (FESC) will be in Adelaide to present at the CSANZ ASM in August.
Julie has over 25 years of cardiovascular clinical research experience, with a special interest in recovery after cardiac surgery including morbidity and patient-reported outcomes. She leads nursing and allied professional research and clinical academic career development at St Bartholomew’s Hospital, one of the largest CV centres in Europe.
Julie is the current Chair, ESC Association of Nursing and Allied Professions (ACNAP) science committee. She also has roles at the Society of Cardiothoracic Surgery (SCTS) Great Britain and Ireland, The Aortic Dissection Charitable Trust (TADCT), and is a founding member of CONNECT, the Cardiac Surgery International Nursing and Allied Professional Research Network.
Make sure you see her presentations at the 2023 CSANZ ASM in Adelaide including:
Thursday 3 August at the Cardiovascular Nurses Symposium presenting all about CONNECT
Friday 4 August at 2.25pm her topic will be “The value of PROs and shared decision making in CVD”
Saturday 5 August at 1.30pm presenting, “Multimorbidity and consequences following cardiac surgery”
Take this opportunity to meet Julie and other nursing leaders who will be presenting at the Cardiovascular Nurses Symposium on Thursday afternoon.
Summary provided by Dr Natalie C. Ward
Elevated lipoprotein (a) [Lp(a)] is now recognised as an independent and causative risk factor for atherosclerotic cardiovascular disease and calcific aortic valve disease, according to the recently released Australian Atherosclerosis Society Position Statement. Elevated Lp(a) is known to be strongly associated with an increased risk of myocardial infarction, stroke, peripheral artery disease, heart failure and cardiovascular mortality. Predominantly determined by genetics, approximately 1 in 5 people have elevated Lp(a) levels, making it the most common inherited monogenic cause of coronary artery disease. In Australia and New Zealand, translating to approximately 5.1 and 1 million people, respectively, which may be further influenced by the multicultural make up of both countries. There is currently limited data available on elevated Lp(a) in Aboriginal, Torres Strait Islander and Māori populations.
It is a continuous relationship between Lp(a) concentration and cardiovascular risk; and it is now recognised that Lp(a) levels >100 nmol/L (>50 mg/dL) are indicative of high-risk within Caucasian populations. While no treatments specifically targeting Lp(a) are currently clinically available, measurement of Lp(a) should be conducted via selective screening of high-risk individuals, to assess and stratify risk. Diet and lifestyle interventions do not have any direct effect on Lp(a) levels, however reduction of all modifiable risk factors, particularly low-density lipoprotein cholesterol (LDL-C) levels via the initiation or intensification of preventative treatments, is crucial for reducing overall cardiovascular risk in both primary and secondary prevention.
Although there are limitations regarding the measurement of Lp(a), methodological advances including the development of assays that are less sensitive to apo(a) isoforms, and standardised reference material have improved its assessment. Other conditions, including impaired renal function, hypothyroidism, menopause, and inflammatory conditions can also impact Lp(a) concentrations. While the focus of this Position Statement is on adults, it is important to note that in children, Lp(a) concentrations vary throughout childhood, only appearing to plateau at 15 years of age. This is particularly relevant when considering cascade testing of relatives of individuals with elevated Lp(a). To assist with implementing measurement of Lp(a) a Medicare Benefits Schedule item for testing and an ICD-10 code for elevated Lp(a) should be established and approved.
The implementation of Lp(a) assessment into routine clinical practice for the prevention of cardiovascular disease will require multiple approaches. Cardiovascular risk calculators incorporating Lp(a) should be developed and validated to improve risk assessment. Patients identified as having elevated Lp(a) should be appropriately referred and have access to consumer-friendly resources that support and communicate the implications of this risk factor. While treatment options are currently limited, personalised care plans are needed to stress the importance of adherence to management of behavioural risk factors and preventative medications targeting modifiable risk factors including hypercholesterolaemia, hypertension, obesity, and diabetes. Advocacy groups of patients and relevant stakeholders also have an important role to play.
By Natalie C. Ward, Gerald F. Watts and David R. Sullivan
Weblink: https://www.heartlungcirc.org/article/S1443-9506(22)01231-8/pdf
A 19 year-old woman presents with palpitations. Continuous rhythm strip post adenosine is shown. What is the likely mechanism of tachycardia? Does this patient need an urgent ablation?
provided by A/Prof Alex Voskoboinik
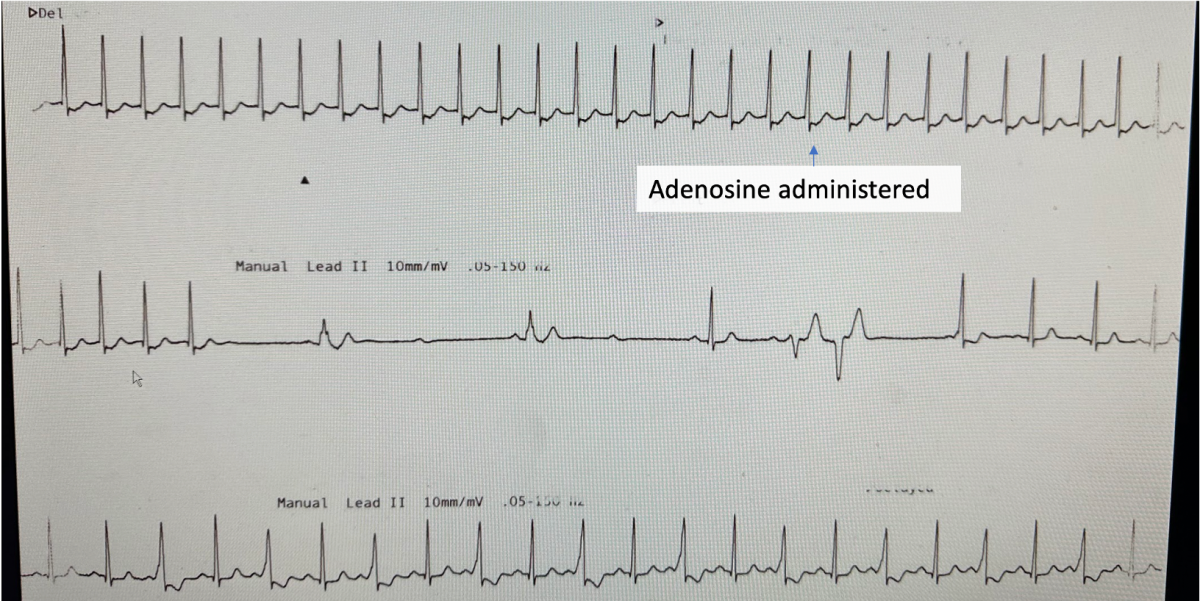
A short RP supraventricular tachycardia is shown initially. Adenosine blocks the AV node and results in termination of tachycardia. This is suggestive of either typical AVNRT and orthodromic AVRT. One notes that the tachycardia terminates with an ‘A’ (seen immediately after the last QRS of tachycardia which would further rule out an atrial tachycardia – where the last abnormal beat is usually a QRS complex; moreover atrial tachycardias are only rarely adenosine sensitive).
Immediately after the tachycardia terminates, the AV node is fully ‘blocked’ and the sinus beats are only intermittently conducted to the ventricle, but down an accessory pathway. These wide complex beats are ‘fully pre-excited’, but some p waves are blocked suggestive the pathway has weak antegrade conduction properties. In the bottom row where adenosine has worn off, one can see that only every second beat is pre-excited (these beats are a fusion of nodal and antegrade pathway conduction) again confirming that the pathway has weak antegrade conduction with a ‘long refractory period’. Hence this would be considered a ‘low risk’ pathway as it is unlikely to be able to conduct AF at rapid rates (which is what can lead to degeneration to VF in patients with WPW). While catheter ablation for SVT should be considered on symptomatic grounds, there is no indication for urgent ablation of this low risk accessory pathway on prognostic grounds.
Pulmonary hypertension (PHT) is known to complicate left heart diseases (LHD) including left sided valvular pathologies such as aortic regurgitation (AR). Patients with significant AR have an increased risk of death, even if they do not have symptoms, so identifying variables which predict adverse outcomes is important. PHT is thought to develop in AR due to left ventricular volume overload which eventually leads to increases in left atrial pressure and the development of post-capillary PHT.
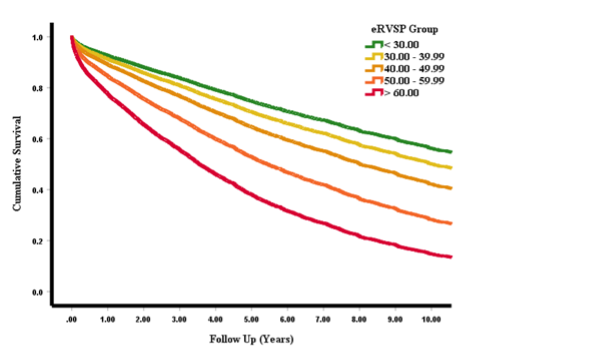
Now published in BMJ Heart, Dr Seshika Ratwatte, senior author Professor David Celermajer and their co-authors identify a cohort of 8392 patients with “isolated” moderate or severe AR and preserved left ventricular ejection fraction (LVEF>50%) using the National Echo Database of Australia (NEDA). The authors show that the risk of all-cause mortality increases as eRVSP level increases even after adjustment for age and sex (Central Illustration), with a ‘threshold’ for mortality seen from mild PHT onwards.
The publication outlines that a significant proportion of the population with significant AR had suspected PHT based on echo. Echo remains the first line screening tool to detect PHT and is the guideline recommended diagnostic method of choice to allow for monitoring and follow up. Clinicians need clear parameters to monitor and prognosticate such patients accurately. The authors identified a typical phenotype of “left heart disease” on echo with E:e’, right and left atrial sizes and the proportion of patients with RV functional impairments increasing progressively, from no PHT to severe PHT.
Central Illustration:
Link to publication is now available in BMJ Heart. https://heart.bmj.com/content/early/2023/04/02/heartjnl-2022-322187

In this edition:
– Intervention for improving acute HF outcomes
– Dapagliflozin in HFimpEF
– Empagliflozin in HFpEF vs. HF with midrange EF
– Intravenous ferric derisomaltose in iron-deficient HF
– Up-titration of guideline-directed medical therapies for acute HF
– Associations of all-cause mortality with statin therapy in HFpEF
– Empagliflozin improves outcomes in HFpEF irrespective of BP
– Combining loop with thiazide diuretics for decompensated HF
– Decongestion with acetazolamide in acute decompensated HF across LVEF spectrum
– Ambulatory haemodynamic-guided management reduces HF hospitalisations
Download Heart_Failure_Research_Review:_Issue_74(pdf) with commentary by Prof Andrew Coats

Join us for the much anticipated CSANZ NZ ASM. Get the team together and head to Auckland in June for 2.5 days of expert lecturers, hands-on workshops, nursing symposium and a range of scientific sessions that will take your knowledge to the next level!
Catch up with old friends and meet new colleagues at the various social activities. Boost your career by presenting your research at the 2023 CSANZ NZ ASM – submit your abstract now!
ABSTRACTS CLOSE ON MONDAY 13 MARCH AT 7PM (NZDT)
R.T. Hall came to Sydney from England in 1853 on the vessel “Waterloo”.
He was consumptive but managed to survive the long voyage and made a complete recovery. His affairs flourished and after he died in 1894, a trust was established initially for: “An invalid home for the reception, cure and treatment of culture for respectable, moral persons, residing in Sydney or its suburbs, and suffering from consumption of the lungs”.
A sanitarium was established in the Blue Mountains in 1909 and was active till the early 1950s when the treatment of tuberculosis radically changed. The trust then looked for an alternative field to support and became involved in The National Heart Foundation. In 1959 and for a number of years, the bequest supported the RT Hall Lecturer. However, in more recent times, the bequest has supported the RT Hall Prize and the lectureship has been funded by a donation from The National Heart Foundation, for which we are very grateful.
Register for the next CSANZ ASM here
